
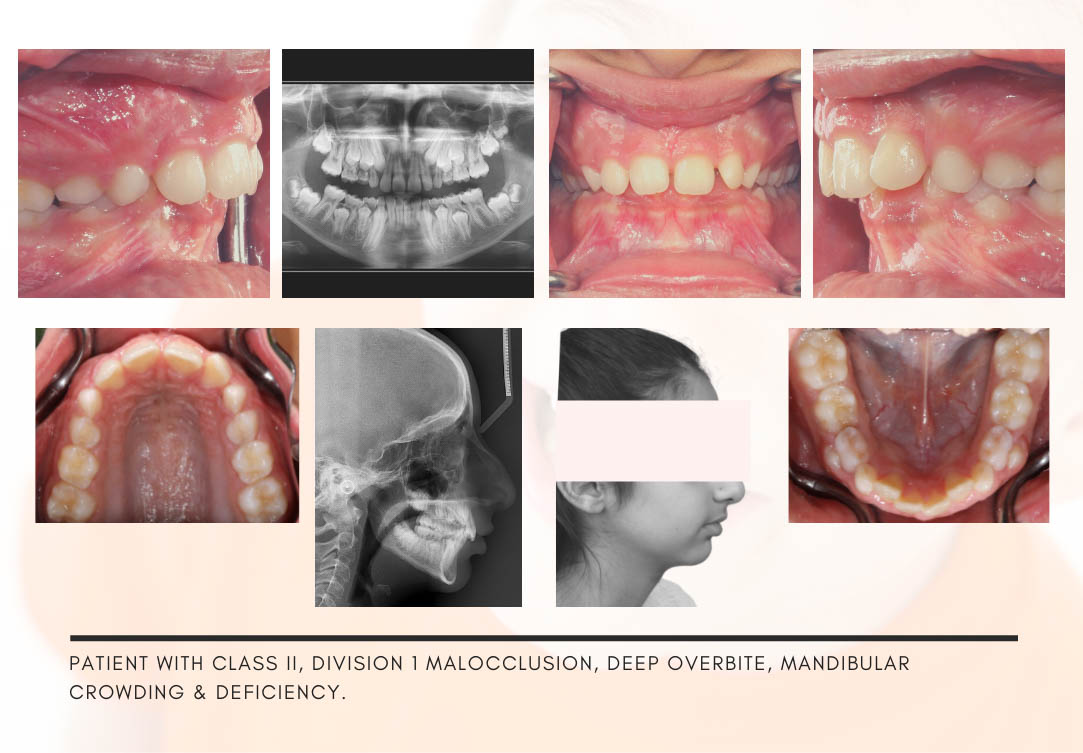
Sometimes when you reach the end of treatment and the upper canines reach the back of the lower canines (class I canine relationship), the patient's overjet does not return to normal. Having a normal overjet at the end of treatment depends on three factors:
• Suitable torque for incisors
• Proportion between the size of the anterior teeth
• Tip the anterior end teeth
By recognizing these factors, you can give a better quality of treatment to your patients. The effect of incisor tooth decay is approximately 40% of the population of class II patients. Lack of proper torque is more common in class II patients, so we will talk about these patients first. In a Class II patient (maxilla anterior or mandibular posterior), we have dental compensations, that is, the upper incisors are retroded and the lower incisors are protruded due to the large axis. In this way, the patient's overjet is reduced to some extent. There are three ways to treat these patients:
1- If the patient is a child (under 13 years old), functional therapies are excellent because they stimulate the growth of the mandible and achieve an acceptable profile. If the patient is over 14 years old, functional treatment is no longer possible due to the end of the period of horizontal growth of the mandible, so you will have the second and third options:
2- If the anterior placement of the mandible makes the patient's face more beautiful, you should wait until after the age of 18 to come forward later with orthognathic mandibular surgery and correct the jaw relationship and make the face more beautiful.
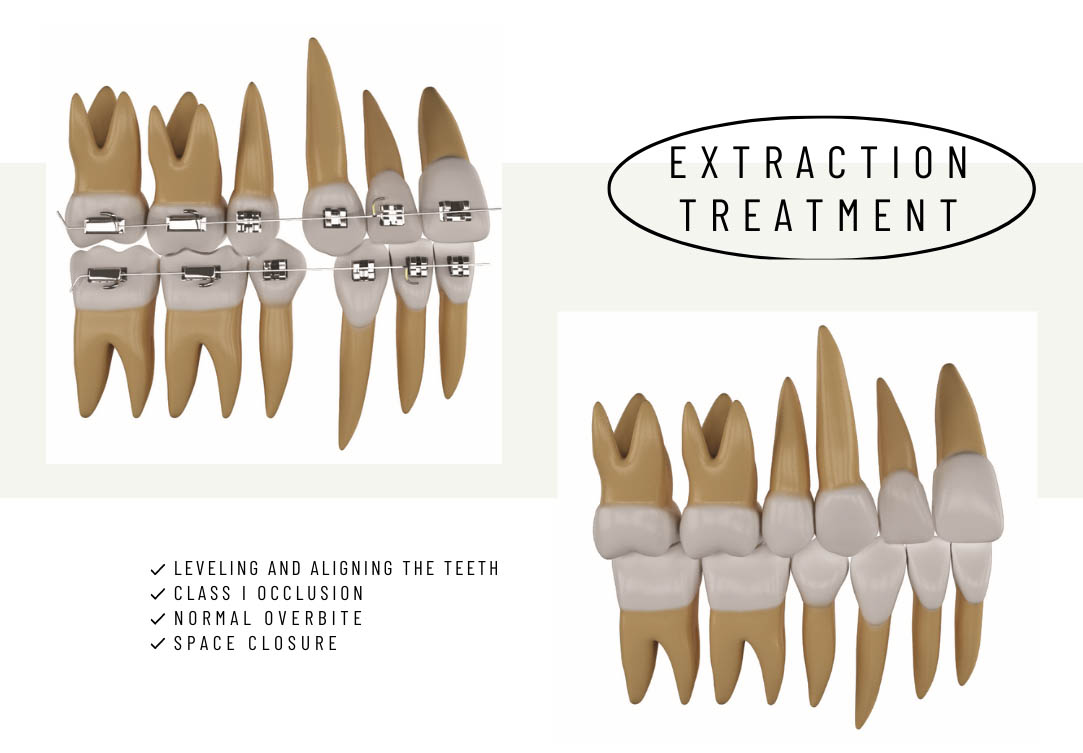
3- In cases where the abnormality is not severe, the upper two premolars can be pulled and the upper anterior ones can be retouched and the patient's overjet can be corrected. In this case, we usually do not pull the lower premolar and finish the treatment of the mandible with a strip or maximum pulling of an incisor. At the end of the treatment of these patients, the molar relationship of a complete class II cusp ends. When removing the above premolars, you must determine the type of anchorage according to the patient's occlusion. However, treatment of this group is associated with distalization of the upper anterior to reach a class I canine occlusion and a complete class II molar cusp.
Due to the Class II jaw relationship (either the upper jaw is forward or the mandible is posterior) we have some dental compensation. Dental compensation in Class II patients is in the form of retrograde of the upper incisors and protrusion of the lower incisors to achieve a better overjet. When the upper incisors are retrograde, that is, their angle with the maxilla is reduced, they are placed in a smaller arc. When the lower incisors are protruded, that is, their angle with the mandibular plane is greater, they are placed in a larger arc. On the other hand, the lower incisors become more protruding as the crucifix smoothes.
After pulling the upper premolars, the upper incisors go back to close the spaces, but because the force is applied to the crown of the incisor teeth, more crowns and less roots go backwards. The above incisors were retrograde due to dental compensation. By pushing them back, it becomes more retrograde and the arc becomes smaller again.
When you reach the end of the treatment and the molar relationship is a complete class II cusp, Hyde and Overjet are also normal, you will see that some space is left in the premolar area. what should we do?
If you move the fronts back to close the space, the incisors will tip to the tip.
If you bring the molars forward to close the space, the correct molar relationship will be lost.
Of course, to maintain the molar relationship, the posterior should not move mesially, so the upper incisors should be pushed back, but what to do with zero overjet.
One of the reasons for facing this situation is the loss of the correct torque of the incisors. The angles of the upper incisors are reduced to the maxillary plane and placed in a smaller arc; The angle of the lower incisors is also increased to the mandibular plane and they are located in a larger arc; Therefore, the patient's overjet is zero and the anterior teeth will not fit.
To treat it, you need to correct the upper and lower incisors, which is possible in three ways:
1. Create some torque in the incision area of the 0.019x0.025 stainless steel arch. This bend in the upper jaw gives rise to the palatal torus to become the palatal root and the buccal crown, and in the lower jaw it gives the root to the buccal torus to the buccal root and crown.
Be lingual.
2. Use 0.021x0.025 nickel titanium or steel arch. The larger the diameter of the R-chowir, the better the torque of the brackets. The 0.019x0.025 archwires inside the 0.022 bracket groove have about 10 degrees of freedom, which is called a slope. Because of this amount of freedom between the R. Chauer and the groove of the brackets, the amount of torque in the anterior brackets is greater than what we see in normal individuals under the study of Mr. Andrews. The actual amount of torque obtained in normal individuals is 7 and 3 degrees positive for the upper central and lateral, respectively, and 1 degree negative both for the central and lateral, respectively, while in brackets 17 and 10 degrees positive for the upper and 6 degrees negative for the lower, respectively. Is considered.
Increasing the amount of torque is to correct 10 degrees of freedom between the archwire and the groove of the bracket, but in cases like the same class II patients, we see that this amount of increase in torque is still not enough.
If you use thicker archwires such as 0.021x0.025, the amount of freedom reaches 5 degrees. The torque of the upper incisors gets 5 degrees better because it is positive, so the root becomes more palatal and the crown more buccal. Torque of incisors below 5 degrees is better because it is negative, so the root is more buccal and the crown is more lingual. This process creates an overjet.
3. The release of 0.019x0.025 nickel-titanium was introduced to the market, which has a torque of 20 degrees in the incisors. You can use these archwires.
In all these cases, it is better to strip the lower incisors so that the crown can be lingualized more easily, and the upper anterior ones should be connected with a 4-figure ligature wire so that there is no distance between them when the crown becomes buccal.
Therefore, if the overjet is reduced due to the loss of torque, you can modify the torque to reach the correct overjet at the end of the treatment.
The effect of anterior tooth size
If the lower forearms are larger, two states will occur or they will protrude, or if they are on the same arch, they will have a cradling state.
On the other hand, if the upper anterior ones are smaller (for example, the upper lateral one is peg-shaped), they will be placed in a smaller arch.
At the beginning of the treatment, the size of the upper anterior or the size of the lower anterior may not be very important, but when you reach the end of the treatment and the upper canine is behind the lower canine, you will no longer have a normal overjet.
Bolton Analysis
There is always a proportion between the size of the upper and lower anterior. Mr. Bolton first discovered this in the 1950s and found that if the size of the lower anterior teeth was approximately 77% of the size of the upper anterior teeth, at the end of treatment, when the upper canine was behind the lower canine, it would reach a normal overjet. For example, if the sum of the widths of the six anterior teeth above is 40mm, the sum of the widths of the six anterior teeth below should be 31mm (31mm = 40mmx0.77). Now, if the size of the lower anterior is more than this, for example, it should be 32 or 33 mm, because they are placed in a larger arch to be arranged, so you will not have a normal overjet at the end of the treatment. You should do this test at the beginning of treatment and find out. If the size of the upper lateral is smaller than normal, it is better to consider this amount for the reconstruction of the lateral crown so that it looks better at the end of the treatment. If the upper lateral size is good, you should strip from the lower anterior.
This stripping has nothing to do with crading. You may have a class II patient who has both jaws in order and only the patient complains of high protrusion and no lower credentials, but his Bolton analysis is disproportionate and the anterior 2mm is larger than allowed. Although the patient does not have crading, you still need to do a lower anterior strip to normalize the overjet at the end of treatment when the canines are class I.
You can strip each lower anterior tooth to 0.5mm, so if this mismatch is up to 3mm, you can compensate with anterior strips, but there are cases where the size difference is more than 4mm, in these cases you pull one of the lower incisors.
Any patient who has some cradling in the lower anterior region should not have an incisor pulled. Drawing a lower incisor in a patient with class I occlusion has the following assumptions:
1- The upper arch should be almost regular and without cradling.
2- Bolton analysis is disproportionate from 4mm up and does not complain of protrusion. It will be normal that at the end of the treatment of these patients, the top and bottom midlines do not overlap because the bottom no longer has a midline. Of course, it does not matter because most of the upper teeth are visible in a smile. (Of course, pulling the incisor down is also recommended in other cases, such as a half-cusp molar relationship up to class II, which we will explain later.)
Some colleagues think that pulling the premolars will solve the problem of cradling, so there is no need for a strip, while the strip is not for cradling but to reach a normal overjet at the end of treatment (analysis).
Bolton) you do. This mismatch between the six upper and lower anterior teeth has nothing to do with the posterior teeth, so if you pull from the premolars, it will not affect the size of the anterior teeth. You have to do the strip.
This belief goes back to a time when we thought strip was only for cradling, and since the premolars were drawn for this purpose, we should not strip anymore. This belief is wrong because strip is used for four different cases. So even if there is no crading, we will strip again because of Bolton, and even if you pull the premolars for cradling, you will still have to strip.
In some patients, there is a complaint of protrusion or a lack of low arch space, and at the same time the Bolton analysis is more than 4 mm disproportionate. Proliferation of the premolars will be necessary in these patients, but what should be done with Bolton analysis? Should both premolars and an incisor be pulled?
No, we can not extract three teeth from one arc. In these cases, pull the lower two premolars to correct the lack of space or correct the protrusion, but to achieve the correct fit of the teeth and the overjet at the end of the treatment, you can strip some of the lower anterior and reconstruct some of the upper laterals. Usually, the large mismatch between the size of the upper and lower teeth is not only related to the size of the lower anterior but also to the small size of the upper laterals.
Reconstruction of the upper laterals is performed after removing the anterior cradle and continuing the laceback to create space between the canine and the lateral.
Usually, there is a lack of overjet at the end of treatment due to the disproportion of the torque and the size of the teeth, provided that you make a class I canine occlusion for the patient. We see a lot of treatments that end the relationship of canines at the end of class II treatment, and it is natural that the amount of overjet will not be low at the end of treatment. It is important that you have a normal overjet when the canines are at the end of Class I treatment.
Tip Effect The anterior teeth end in a smaller arch when the teeth are upright until their crown
It becomes mesial. The more mesial the crown, the larger the arch.
The upper anterior brackets (central, lateral and canine) on the left and right have a total of 40 degrees Tip, while the lower anterior brackets on the left and right have a total of 6 degrees. For this reason, the upper anterior are placed in a larger arch than the lower anterior. As mentioned, due to the torque and the size of the teeth, you will have a small overjet mainly at the end of the treatment, so with the changes in the tip of the brackets, you will make some overjet so that they do not need to strip the teeth too much for the overjet problem.
So we conclude that the following three factors play a role in building an overjet at the end of treatment when the canines are class I:
• Torque incisors
• Proportion between tooth size
• Anterior tip
The anterior tip is in favor of building an overjet, while the first one or two will reduce the overjet. So always do a Bolton test at the beginning of treatment. If you see a mismatch (size of the lower anterior or small anterior), do two things:
A. Lower anterior strips
B. Reconstruction of the upper lateral crown (this condition is possible in extensible patients and is usually not possible in non-extensible patients.)
Once you are sure of the fit of your teeth, you start the treatment until the end of the treatment. At the end of the treatment, if you encounter a lack of overjet again, it must be due to the torque of the incisors, and the way to treat it is to use new wires with 20 degrees of torque.
Posterior end bracket tip The back bracket tip in the MBT method has nothing to do with the current topic (having a normal overjet) but knowing it is not without merit.
The reason why the upper premolars are made with a zero degree tip is to be in the upright position and to pass through the lower premolars in lateral movements.
The premolars and lower molars are made with a two-degree tip to make the crown slightly mesial. A large percentage of your patients are class II, and lower posterior crown mesentery helps to achieve class I occlusion. On the other hand, in class I patients, when the premolars are pulled, the upper posterior ones (due to having spongy bone and the fact that the upper anterior ones have larger roots than the lower anterior ones) are more mesile than the lower posterior ones, so at the end of treatment . For this reason, the lower back is made with more tip than the upper to make it easier to reach the posterior class I occlusion.
If you are treating a Class III-prone patient, it is best to attach the canine bracket and lower left premolars to the right and right to left to tip negatively and distal the crown to achieve Class I occlusion sooner.
Tip The upper canine is made 8 degrees to give the crown of the upper canal and the upper canopy overlap. In this way, in lateral movements, it will have a good contact with the lower canine to reach the occlusion of Caspian rise





































 March 07, 2022 - توسط مدیر
March 07, 2022 - توسط مدیر